

Hemophagocytic lymphohistiocytosis (HLH) is a potentially fatal hyper-inflammatory disease induced by aberrant immune activation and subsequent proliferation of macrophages, histiocytes and T-helper cells. In this abstract we present a case of HLH, which relapsed twice despite ongoing treatment, and we hypothesize on possible causes and mechanisms.
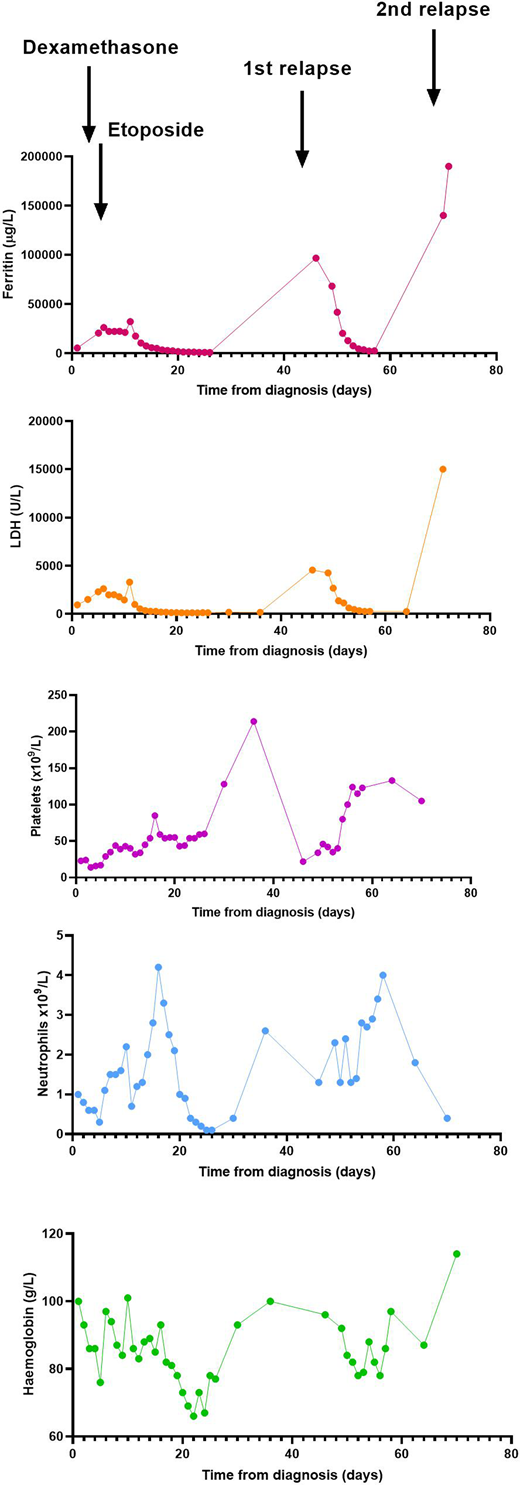
A 77 year old female presented to our hospital with ongoing fevers and worsening cytopenia. Blood counts from three years before the current presentation showed Hb 120g/L, WBC 4.0 x 10^9/L, Neutrophil count 1.8 x 10^9/L, Lymphocytes count 1.8 x 10^9/L and Platelet count 104 x 10^9/L. A bone marrow examination at that time revealed a normocellular marrow with 28% lymphocytes of which70% were CD 4+, CD 3+, CD5+ and CD 7-. Molecular studies confirmed T cell receptor (TCR) gamma gene rearrangement. The karyotype on the bone marrow was normal. In the absence of clinical symptoms, the patient was regularly followed up without specific therapy. During the current admission, however, the patient was febrile, had progressive pancytopenia and biochemistry suggestive of HLH (Fig 1). She was extensively evaluated which ruled out infective and malignant causes.
A bone marrow aspirate and biopsy was performed and treatment initiated as per HLH-94 protocol. The bone marrow examination showed marked features of haemophagocytosis on a normocellular background. A small clone of T-lymphocytes was again noted with similar features as in the first biopsy. In addition, a prominent population (10%) of promonocytes was apparent with an uncertain significance. Karyotype was normal. Next Generation Sequencing showed TET2 frame shift mutation at low variant allele frequency (5%).
Patient responded well to treatment. While on tapering dose of steroids, the disease flared up (Fig 1) and the patient was restarted on high dose steroids with etoposide. After a quick initial response, while still on active treatment, she again relapsed within 3 weeks, coupled with sepsis and acute myocardial ischemia, followed by sudden death.
We were unable to identify a cause for HLH. There were 10% promonocytes in bone marrow and evidence of aberrant T-cells on flow cytometry. Although there was no obvious evidence of dysplasia on microscopy, the flow cytometry showed up- regulation of CD 64 and CD 14, down regulation of CD13 and 11b, and CD 34 expression in granulocytes possible indicating dysplasia as per the Wells criteria. (Wells et al., Blood 2003; 102(1):393) The Next generation sequencing showed TET2 mutation as mentioned above. Mutations in TET2 have been found to have overrepresented in chronic myelomonocytic leukemia in as much as 50% of patients and around 20-35% of patients with myelodysplastic syndrome (MDS). These patients with TET2 mutation have been found to have altered methylation. Recently TET2 has been implicated in immune regulation with evidence of abnormal CD 4 T cell proliferation (present in our patient) and disruption of T cell homeostasis. In addition, patients with TET2 mutation associated myelodysplastic syndrome are known to have auto-immune manifestations (Yimei Feng et al., Frontiers in Oncology, 2019 (9):1).
Alyssa H et al have shown that TET2 mutant in patients with MDS (Myelodysplasia) leads to alteration of immune environment in the macrophage differentiation (Alyssa et al., Experimental Hematology, 2017:55; 56). Whether these immune aberration caused recurrent florid relapse of hemophagocytosis in our patient within a span of 2-3 months remained unclear and it could be considered in future research. Even though the occurrence of hemophagocytic syndrome has been described in acute leukemias, the association of the same with myeloid gene aberrations with or without overt myelodysplastic features is unknown. However since hemophagocytosis itself is not common, a careful evaluation to look for uncommon associations which may be a triggering factor may pave the way for identifying their possible role in the pathogenesis. And therapeutic options such as hypo methylating agents can evolve when such associations are confirmed in future studies.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal